First Trial - Study Details
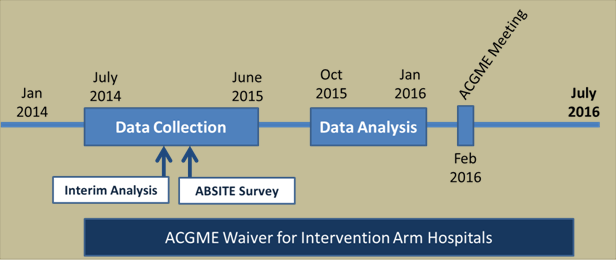
First Trial Timeline (2014-2016)
Summarized Results
Patient Outcomes
Patient outcome analyses were performed on 138,691 general surgery patients. The rate of death or serious complication did not significantly differ between study groups (9.1% in the flexible-policy group and 9.0% in the standard-policy group, P=0.92). In regards to other secondary patient outcomes, the flexible-policy group was found to be noninferior to the standard-policy group for serious complications, any complication, unplanned reoperation, sepsis, surgical-site infection, and urinary tract infection.
Resident Outcomes
Resident outcomes were analyzed for 4,330 general surgery residents. There was no significant difference in resident satisfaction with overall education quality (11.0% in the flexible-policy group and 10.7% in the standard-policy group, P=0.86) or resident satisfaction with overall resident well-being (14.9% vs 12.0%, respectively; P=0.10). Residents in the flexible-policy group compared to the standard-policy group were less likely to be dissatisfied with continuity of care (odds ratio 0.44; 95% CI, 0.32 to 0.60; P < 0.001) and quality and ease of handoffs and transitions in care (odds ratio 0.69; 95% CI, 0.52 to 0.92; P=0.01), and less likely to perceive a negative effect of institutional duty-hour policies on patient safety, continuity of care, clinical-skills acquisition, operative-skills style="line-height: 1.4em;" acquisition, autonomy, operative volume, availability for elective and urgent cases, conference attendance, time for teaching medical students, the relationship between interns and residents, and professionalism (all odds ratios>1.00, P < 0.001 for all comparisons except P=0.003 for professionalism). There were no differences in ABSITE or board examination scores between study arms.
In contrast, the flexible-policy group was more likely to be dissatisfied with time for rest (odds ratio 1.41; 95% CI, 1.06 to 1.89; P=0.02) and perceive negative effects of duty hour policies on resident outcomes that depend on time away from the hospital (odds ratios >1.00, P < 0.001). However, most of these concerns decreased as residents progressed through their residency. In fact, compared to interns, overall well-being was significantly better in the flexible-policy group for PGY2-3s, and even more so for PGY4-5s.
When residents were asked what proportion would choose a standard-arm policy program vs a flexible-arm program if they could go back in time, only 14% preferred standard policy.
Finally, it could be that cumulative years under flexible duty hour policies would result in worse patient outcomes and worse resident wellness. In examining the long-term results of the FIRST trial, we found that there was no significant change over time in resident well-being or patient outcomes. Flexibility continued to have a positive impacts on continuity of care.
ACGME Policy Changes
Accordingly, after a period of detailed review, the ACGME revised duty hour requirements in accordance with the flexible duty hour requirements utilized in the FIRST Trial beginning July 1, 2017.